There is already a great deal of knowledge about what sorts of processing go on where in the brain, and no lack of speculation about how and why. An excellent and detailed survey for a lay audience can be found in William H. Calvin and George A. Ojemann's CONVERSATIONS WITH NEIL'S BRAIN . If you are curious (and most people find the topic fascinating), you should spend some time reading either the on-line version or the published version of this book.
Much of the information that we have comes from studies of the functional consequences of localized brain injury, mostly due to stroke. Although the taxonomy of language-related brain injuries has been elaborated over the past decades, the basic categories remain those that were identified by two 19th-century researchers, Paul Broca and Carl Wernicke.
As a National Institutes of Health information page says:
A note of caution: functional localization varies, sometimes considerably, across individuals. Brain injury (most commonly caused by stroke) is usually widespread enough to affect several different functional areas. Thus each patient is individual both in terms of symptoms and in terms of the correlation of symptoms to area of damage. Nevertheless, there are broad syndromes of deficit-associated-with-local-damage, as described succinctly in the NIH passage above, that are characterized as Broca's and Wernicke's aphasia.
Here is a somewhat more precise picture of the typical placement of Broca's area and Wernicke's area relative to various landmarks of cortical anatomy and physiology:
Broca's aphasia is sometimes called disfluent aphasia or agrammatic aphasia. It is named after Pierre-Paul Broca (1824-1880), a French surgeon and anthropologist who first described the syndrome and its association with injuries to a specific region of the brain.
Agrammatism typically involves laboured speech, and a lack of use of syntax in speech production and comprehension (although patients who present with agrammatic production may not necessarily have agrammatic comprehension).
An example of agrammatic speech:
Examiner Keep going.
M.E. Scrubbed and uh washed and un...tidy, uh, sisters and mother, prince, no, prince, yes. Cinderella hooked prince. (Laughs.) Um, um, shoes, um, twelve o'clock ball, finished.
Examiner So what happened in the end?
M.E. Married.
Examiner How does he find her?
M.E. Um, Prince, um, happen to, um...Prince, and Cinderalla meet, um met um met.
Examiner What happened at the ball? They didn't get married at the ball.
M.E.No, um, no...I don't know. Shoe,
um found shoe...
In between the motor strip and Broca's area are the areas
known as the supplementary motor area (SMA) and the premotor cortex, which
are said to be involved in the generation of action sequences from memory
that fit into a precise timing plan All in all, it seems likely that Broca's
area is connected to serialization of coordinated action of the speech
organs. Why do certain syntactic abilities also seem to be localized there?
Perhaps a neural architecture evolved for creating and storing complex
motor plans has been pressed into service to create and store symbolic
rather than purely motoric structures. As Deacon (1991) writes:
Wernicke's aphasia is sometimes called sensory aphasia or fluent aphasia. The speech of a Wernicke's patient is often a normally-intoned stream of grammatical markers, pronouns, prepositions, articles and auxiliaries, with difficulty in recalling correct content words, especially nouns (anomia). Words may be meaningless neologisms (paraphasia).
The patient in the passage below is trying to describe
a picture of a child taking a cookie.
Examiner Yeah, what's happening there?
C.B. I can't tell you what that is, but I know what it is, but I don't now where it is. But I don't know what's under. I know it's you couldn't say it's ... I couldn't say what it is. I couldn't say what that is. This shu-- that should be right in here. That's very bad in there. Anyway, this one here, and that, and that's it. This is the getting in here and that's the getting around here, and that, and that's it. This is getting in here and that's the getting around here, this one and one with this one. And this one, and that's it, isn't it? I don't know what else you'd want.
Wernicke's area is related to the parietal lobe association cortex, where cross-modality integration is performed, and is adjacent to the auditory association cortex. Thus Wenicke's aphasia is sometimes called a "receptive" aphasia, by distinction with the "production" aphasia of the motor-system-related Broca's syndrome. However, as the above examples indicate, Wernicke's patients show plenty of problems in producing coherent discourse. Even if Wernicke's area originally served a receptive function, it has been taken over by the linguistic system just as Broca's area has been.
To give you some sense of what the injuries involved in
this aphasic syndromes are like, here is a photo of the excised brain of
a Wernicke's patient:

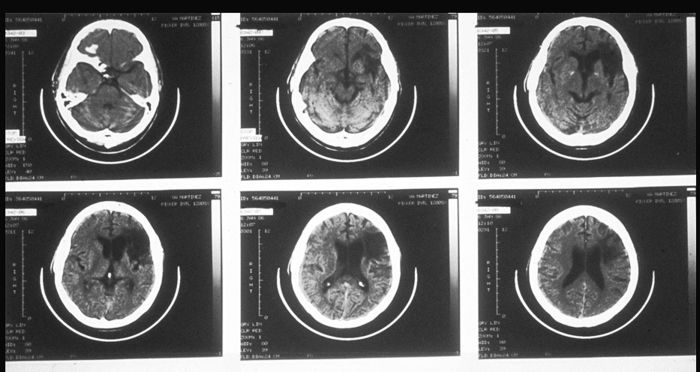
Here is a set of tomographic pictures of a different Wernicke's syndrome brain. The front of the head is towards the top, and the dominant (left) side is on the right, so it is as if we are looking at the brain from the bottom:
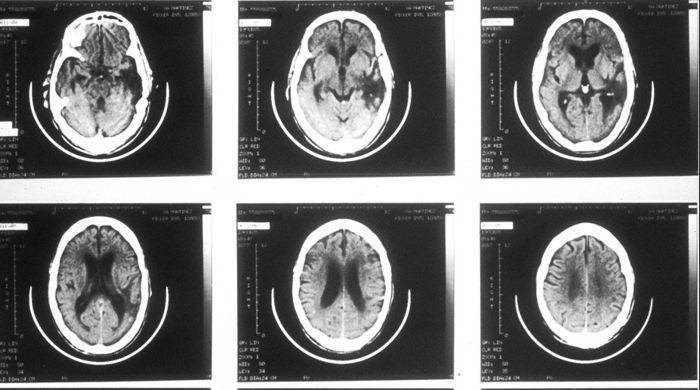
Here is a similar set of tomographic pictures of the brain of a Broca's patient: